Anti-aromatases are a group of drugs used in athletes to counteract the side effects of steroids, namely the increase in estrogen.
Preamble: what is estrogen?
Estrogens are a group of hormones whose function, in their natural state, is to be a primary female sex hormone. They are produced primarily by the development of the follicles of the ovaries and by the placenta. Some estrogens are also produced in small amounts by other tissues such as the liver, adrenal gland, breasts and fatty tissue. These secondary sources of estrogen are particularly important for women in the post-menopausal period.
The three natural estrogens are estradiol, estriol and estrone. In the body, they are all produced from androgens under the effect of aromatase enzymes. Estradiol is produced from testosterone and estrone from androstenedione. Estrone is much less potent than estradiol, and in post-menopausal women there is more estrone than estradiol.
Although estrogen is present in both sexes, it is found in significantly greater amounts in women than in men.
In addition to their role in female and male reproduction, estrogens are involved in the development of the central nervous system, in homeostasis (physiological process, allowing to maintain certain constants of the internal environment of the organism) of the skeleton and the cardiovascular system. They also have effects on the liver and adipose tissue.
What are the reference values for humans?
Estradiol levels are relatively low in men. Before puberty, it is lower than 0.13 nmol/l, while in adulthood it is between 0.08 and 0.18 nmol/L, i.e. 22 and 49ng/L, before dropping to between 0.04 and 0.18 nmol/L in the third age.
Note from Thor49: the optimal level for a bodybuilder should be between 20 and 29ng/L
It is known that too much estrogen disrupts the androgen balance of the male endocrine system. When this balance is disturbed, there is a high chance of developing gynecomastia.
Note from Thor49: I would only talk about estrogen-related gynecomastia and not prolactin-related gynecomastia here.
What does gynecomastia consist of?
Gynecomastia is the excessive development of mammary glands in men. It can be congenital or due to disease, tumor or certain medications (anabolic steroids, androgens, anti-androgens, tranquilizers, antibiotics, chemotherapy, heart medications and medications used to treat AIDS). It can affect one breast (unilateral gynecomastia) or both (bilateral gynecomastia).
The development of the mammary gland is due to an imbalance in the androgen/estrogen balance in favor of the latter.
This imbalance can be explained by:
- A decrease in testosterone (e.g. central or peripheral hypogonadism, primary or acquired);
- An increase in SHBG (Sex Hormone-binding globulin) which leads to a relative decrease in the free, and therefore active, form of testosterone (this is the case in hyperthyroidism, certain liver diseases);
- An increase in estrogen (in certain forms of testicular cancer or in cases of excessive aromatization (chemical transformation of estrogen precursors into estrogen) in peripheral fatty tissue or in hyperthyroidism or Klinefelter’s disease*);
- Androgen receptor inefficiency (secondary to treatment);
- A displacement of estrogen from its receptor (SHBG) by a molecule, thus increasing the free form of this hormone (case of certain drugs).
PS: Kinefelter’s disease: 47,XXY is an aneuploidy that is characterized in humans by an extra X sex chromosome. The individual then has two X chromosomes and one Y chromosome, that is 47 chromosomes instead of 46. The individual is then of male character, but infertile. Its chromosomal formula is written “2N=47, XXY”, not “2N=46”.
PS2:Aneuploidy characterizes a cell that does not have the normal number of chromosomes.
Are we only risking gynecomastia?
In addition to the physical aspect (“breast” growth), an estrogen level that is too high or too low can result in other symptoms such as :
non-exhaustive list
* loss of libido and erections
* belly flab
* fatigue, loss of dynamism
* muscular degradation
* bad mood
* night sweats
* depressive tendency…
What are the different anti-aromatases?
Nolvadex or Tamoxifen Citrate
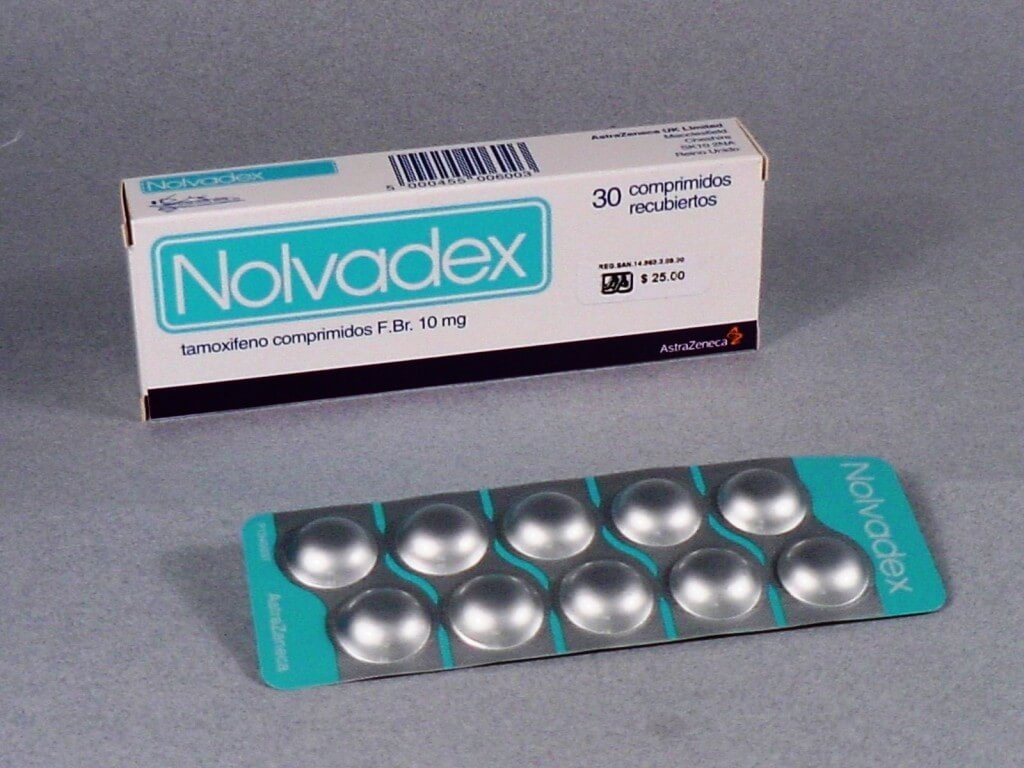
Dosage:
20mg to 40mg/day
Nolvadex acts as an estrogen antagonist by preventing estrogen from binding to estrogen receptors (SERMs).
Nolvadex is most often used in PCT (Post Cycle Therapy) in combination with Clomid, for example, by restarting testosterone production in the testicles.
Best time of use: The best time to use this SERM is during PCT. Indeed, its action on the pituitary gland (hypothalamus) is very useful during this critical moment.
As a reminder, clomid and nolvadex both act on the axis but in opposite ways.
Proviron or Mesterolone

Dosage:
25mg/day for men to 100mg/day.
Proviron is a synthetic, orally effective androgen that has no anabolic characteristics. Proviron is used in medicine to alleviate or suppress disorders caused by a lack of testicular hormones.
Proviron is an estrogen antagonist that prevents steroid aromatization. Unlike Nolvadex, which only blocks estrogen receptors, Proviron prevents steroids from aromatizing. Therefore, gynecomastia and water retention are successfully blocked. Since Proviron strongly suppresses estrogen production, no rebound effect occurs after discontinuation of treatment as is the case with, for example, Nolvadex, where steroid aromatization is not counteracted. It can be stated that Proviron treats the problem of aromatization at its root while Nolvadex simply treats the symptoms. With Proviron the athlete gets more muscle hardness since the androgen level is increased and the estrogen concentration remains low.
Note from Thor49: I like Proviron a lot during a cure with 19nor like deca-durabolin or trenbolone, It is also very useful during a competition for the hard aspect. For the latter case the dose can be between 75 and 100mg/day.
Anti-aromatase inhibitors
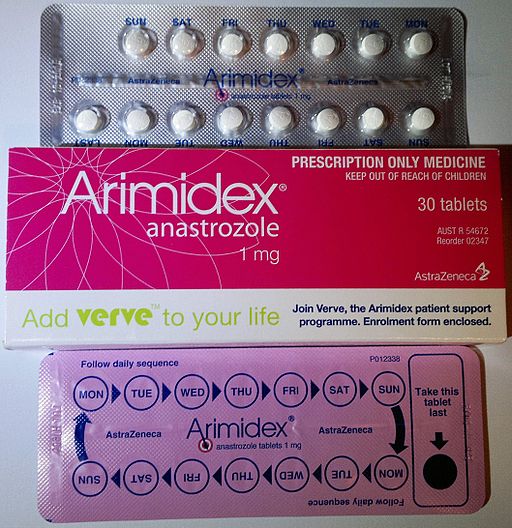
Arimidex or Anastrozole
Dosage:
Between 0.25mg, 0.50mg, 1mg/day or E2D or E3D
Arimidex contains Anastrozole as the active ingredient. The function of this drug is to inhibit the enzyme aromatase, which is associated with the production of the female sex hormone, estrogen.
Arimidex (anastrozole) was the first selective aromatase inhibitor used in bodybuilding, and is still the most popular estrogen regulator
Arimidex overdose results in abnormally low estradiol levels and typical side effects of joint pain, reduced libido, and/or gastrointestinal distress. The first two effects are directly caused by low estradiol levels. Possible side effects of Arimidex exist and come in different forms. This can often be headaches, nausea and vomiting, mood disorders, exhaustion or fatigue.
Appropriate time of use:
During a steroid cycle especially if the dose is greater than 750mg per week (including testosterone and ASA).
Letrozole or Femara
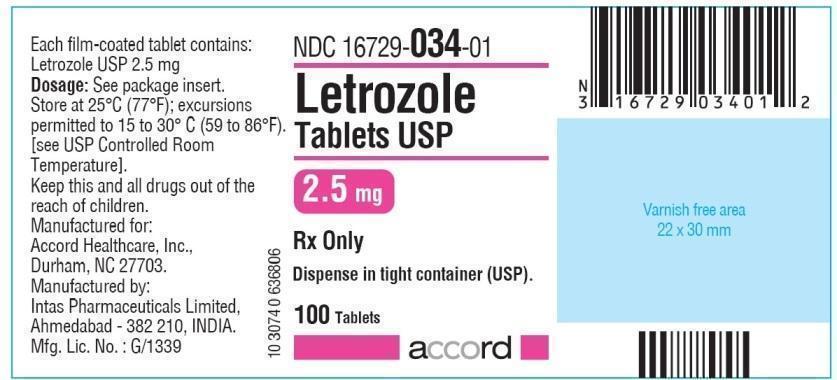
Dosage:
0.36 mg/day never more than 1mg/day
Letrozole is the second anti-aromatase inhibitor in the class. This AI is used in the case of an existing gynecomastia. Letrozole can accomplish the desired effects exactly as intended, with even a better side effect profile – essentially none when properly dosed – than either Arimidex or Aromasine.
Note from Thor49: It is important to take into account the half-life of the drug which is 2 days. If you are taking this type of product to quickly reduce the ES of gynecomastia, it is better to double or even triple the dose on the first day in order to reach the dose that the body needs quickly.
As is often the case with CEWs, there are side effects. Thus the risks of muscular tears are important, tendinitis is also very frequent.
It is also possible to be confronted with skin problems with a strong development of acne but also impotence, headaches, liver problems etc…
Best time to use: During a steroid cycle, especially if the dose is greater than 750mg per week (including testosterone and ASA). It is especially useful in the competition phase to give a harder look!!!
Aromasine or Exemestane

Dosage: 12.5 to 25mg EOD, E3D or E4D
Exemestane is an aromatase inhibitor and is categorized as a “steroidal suicide”. This is where it differs from Letrozole and Arimidex. It is very similar in structure and action to formestane, although it is significantly more potent in comparison.
Aromasin, as it is most often called, is a very powerful AI that works by blocking the aromatase enzyme in the body. Although not as strong as letrozole, aromasin is considerably stronger than anastrozole. Studies with this substance generally show an 85% to 98% reduction in estrogen levels in the body. Unlike Arimidex and Letrozole, which work by reversibly blocking access to the aromatase enzyme, Aromasine deactivates the enzyme molecules one by one when bound to them.
For my part, this is the only CEW that we will start using the same day we start the cycle. It is also important to note that Aromasin has been shown to be very effective in increasing testosterone and IGF levels in the body. Because of this, this drug is also very useful during PCT when trying to restore natural testosterone levels to avoid a post-cycle “crash”.
Exemestane reaches peak plasma concentrations within 2 hours of oral administration of a 25 mg dose. The active life of the drug is between 24 and 30 hours. This is significant because it is much shorter than for non-steroidal inhibitors. A single oral dose of 25 milligrams of exemestane causes a relatively long-lasting reduction in plasma and urinary estrogen levels, with maximum suppression occurring approximately 2-3 days after administration and persisting for approximately 4-5 days
Note from Thor49: There are three main reasons to prefer Exemestane during a cycle.
*The molecule has the possibility of being assimilated by the anabolic receptors at only 0.28%, leaving all the room for the anabolic agents during the cycle.
*Another effect of Aromasin is that it acts as a controller of SHBG (see Proviron) which allows the anabolic agents to be more effective during the cycle.
*Some users may even experience an increase in FSH (Follicle Stimulating Hormone).
Conclusion
I sincerely believe that Nolvadex should be reserved for MDT in its capacity as a SERM and the fact that it acts on the pituitary axis.
Letrozole and Arimidex are excellent anti-aromatases. Both have side effects that an informed user will recognize. Letrozole is VERY effective in existing gynecomastia but it is very hard on the concentration of fluid in the body, risking injury.
Arimidex is often mismanaged by some when all that is needed is to take it lying down or to space out the doses.
Proviron is not a “true” estrogen blocker. So I would choose it as an adjunct rather than a full-fledged AI. It has fallen into disuse whereas it has its place during a cycle. I highly recommend it for a cure with a 19nor (deca, npp, tren).
As for the Aromasin, it is a little (a lot?) my favorite. Its use is double thanks to its action on the SHBG. It can also be used in PCT, which is not negligible. As with each of the above products, care must be taken to find the right dosage.
Thor49, any final words?
The dose of AIs should be found through regular blood tests during a cycle. I place a lot of importance on this point because too much or too little estrogen can be very harmful both physically and morally. These products are far from being harmless and like many things, it is necessary to find the right balance of testosterone and estrogen in order to get the most out of the treatment.